The Starting Point
One source of truth, mapped with the SME.
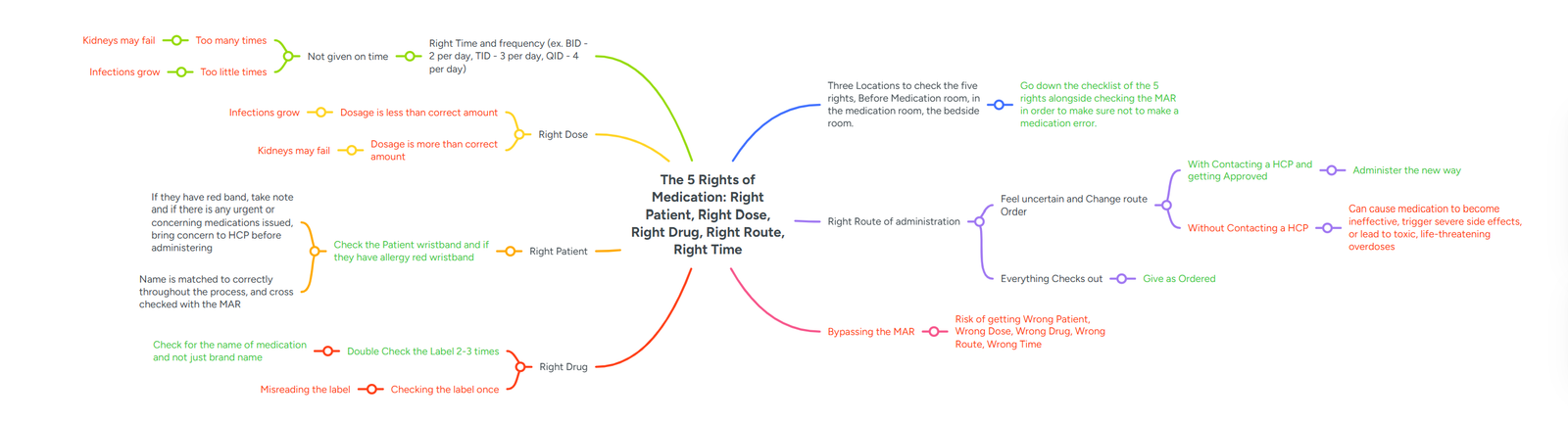
The clinical logic began as a concept map built with the subject matter
expert: each right, its correct action, and the real harm of getting it wrong
(under-dose and infections grow; over-dose and kidneys may fail). It became
the source of truth every scenario was written against.